The complexity of youth AOD practice requires overarching frameworks that enable practitioners to make accurate assessments and apply effective interventions that are timely and commensurate with the goals of clients and others involved in their care.
Youth AOD services seek to address the severity of harmful substance use and the interrelated psychosocial complexity their clients. As such intervention matching and treatment planning requires two structured frameworks; one that enables practitioners to identify and respond to a client’s readiness to address substance use issues (the ‘Stages of Change’) and another that informs effective interventions to address psychosocial problems that both act as determinants of substance use problems and are exacerbated by harmful substance use (the Framework for Resilience-based Intervention). As this a specialist AOD module, the focus will be on using the ‘Stages of Change’ to inform intervention matching and treatment planning.
The Transtheoretical Model of Change
The Transtheoretical model explains change as a process that unfolds over time rather than an event. Understanding a young person’s motivation and readiness to change can inform the formulation of more meaningful and efficacious interventions that can be employed to facilitate change (Miller and Rollnick, 2002). The three interrelated components of the transtheoretical model are:
- The ‘Stages of Change’ delineates a series of five stages that people move through as they change. Each of the stages denotes a certain orientation toward change that will be reflected in the decisions a young person makes regarding their substance use. By examining these decisions youth AOD practitioners can gauge a young person’s motivation to change.
- The ‘Processes of Change’ are ten cognitive and behavioural activities that facilitate the movement of people through each of the stages.
- The ‘Levels of Change’ consist of areas of an individual’s life (i.e. intrapersonal, interpersonal and/or situational) that influence and are influenced by changes. The ‘Levels of Change’ represent complicating problems that can hinder change but if worked through can reinforce healthy change over the long term. They are not explored in this module as they relate more to the framework for resilience based intervention.
The Stages of Change Model
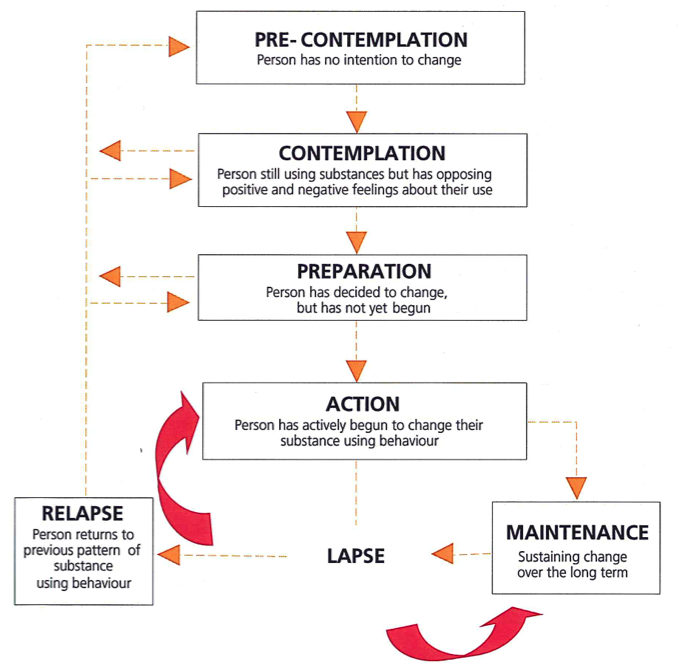
Adapted from: Prochaska, J. & DiClemente, C. (1986). Towards a comprehensive model of change. In: W. Miller & N. Heather., Treating addictive behaviours: Process of change. New York: Plenum Press.
Prochaska, DiClemente and Norcross (1992) identify 10 processes of change (see below); the first five are experiential while final five are behavioural in nature.
The Processes of Change
Experiential processes
Consciousness Raising [Increasing awareness] involves increased awareness about the causes, consequences and potential ways of dealing with problematic substance using behaviourDramatic Relief [Emotional arousal] involves people being moved emotionally by the impact of substance use in their lives. This might stem from a growing or sudden awareness of the connection between their actions and consequences experienced as negative. Strong grief reactions often result which, if dealt with constructively, can be a catalyst for change.
Environmental Re-evaluation [Social reappraisal] combines both affective and cognitive assessments of how substance use impacts on one's social environment.
Social Liberation [Re-engineering] requires an increase in social opportunities or alternatives especially for people who are relatively deprived or oppressed.
Self Re-evaluation combines both cognitive and affective assessments of how substance use shapes one's self-image and one’s image in the eyes of others.
Action oriented / Behavioural processes
Stimulus Control removes cues or triggers for unhealthy substance using behaviour and adds prompts for healthier alternatives. It involves creating the conditions that support change and reduce risks for relapse.Helping Relationships [Supporting] provide support for the healthy behaviour change. These relationships most commonly feature openness, trust and acceptance.
Counter Conditioning [Substituting] requires substituting problematic substance use with rewarding healthy behaviours.
Reinforcement Management [Rewarding] provides predictable consequences for taking steps in a particular direction. This includes both rewards and punishments. Philosophically, the Transtheoretical model orients practitioners to working in harmony with how people change naturally. This involves enabling young people to understand the logical consequences of particular decisions, actions and consequences.
Self-liberation [Committing] relates directly to the belief that change is possible stemming from both enhanced self efficacy and the perception that social and environmental are conducive to change. Self-liberation involves a continuous process of committing to act on the belief that change is beneficial and possible.
The first five ‘experiential change processes’ have been demonstrated to be most effective for application with people in the pre-contemplation or contemplation stages. They accord with non-confrontational interventions that are delivered with empathy and take account of each young person’s perspective. Alternatively, processes that are behavioural in nature (i.e., counter-conditioning, stimulus control, contingency management) have been found to be more effective for individuals in the preparation, action or maintenance stages. These processes accord with action-oriented interventions that focus on the development of skills and strategies that support and reinforce change.
Passive, non-action oriented approaches applied with people in later stages of change are likely to be counterproductive. Conversely, applying action-oriented, behavioural approaches with people in the pre-contemplation or contemplation stages is likely to elicit uncooperative responses. “Confronted with the need for change, an ambivalent person naturally responds with the other side of the decisional balance, with the end result being a misinterpretation of this response as ‘denial’ or ‘resistance’” (Giovazazolias & Davies, 2005; p174).
