Young alcohol and other drug (AOD) users are a heterogeneous population with diverse interests and needs. The usage patterns of different groups can convey nuanced expressions of identity around ethnicity and particular forms of masculinity, femininity or sexual preference. Behaviours that are typical for young people undertaking an adolescent transition are often mistaken as drug related. For example:
- Being rude
- Testing limits
- Demanding more
- Having mood swings
- Having a sudden change in appetite or energy level
- Changing peer group
- Becoming a part of different sub-cultures (Mentha, 1999; p31).
Most young people will experiment with alcohol and potentially other drugs at some stage (Bruun, 2008). Steinberg and Morris (2001) distinguish between occasional experimentation and enduring patterns of dangerous or troublesome behaviour. “Many prevalence studies indicate that rates of occasional, usually harmless, experimentation far exceed rates of enduring problems” (ibid p.90). Even though experimentation can be reckless at times, and binge-style patterns of AOD use can create great risk for adolescents, the majority will go on to develop an ongoing pattern of use that is relatively harmless.
Developmental considerations
Each young person’s stage of development and level of maturity have a bearing on the way they use alcohol and other drugs. It is useful to consider the extent to which the AOD use of young people is influenced by the characteristics of different adolescent sub-stages (even with the limitations described earlier in this section). Bruun and Palmer (1998) offer the following as a guide for the general youth population.
Early adolescence (10 to 13/14)
At this stage young people’s AOD use is often experimental and determined by the substances available in immediate proximity and easily available (e.g. inhalants, alcohol, etc). All substance use (except inhalants) is illegal for young people in this age range. Using is most likely to begin as a shared experience with peers, usually of the same gender. AOD use can be a passport to membership of a group, providing status and an opportunity to be seen as mature.
Mid-adolescence (14 to 17/18)
Due to increased ability to procure drugs through a broader social network, greater autonomy and mobility, young people at this stage are most commonly using for a particular effect. This means that poly drug use is more common. Increased confidence can also mean more risk taking and further experimentation. Socially, AOD use can be a means to status with some peer networks and/ or connecting with potential sexual partners. For young women in this stage, the connections will often be with older adolescents. All AOD use (except inhalants) continues to be illegal.
Late adolescence (18 to 21)
Young people may continue to use substances in a similar manner to the mid-adolescent group but in general, by this stage, will have settled on one or more drugs of choice and a pattern of use. Naturally, this is subject to change. Drug choice will often be the result of relationships developed in new social circumstances such as work or study.
Young people who use substances tend to be strongly invested in the notion that for them, using is an active choice over which they are able to maintain control (Guttierrez & Palacios, 2004). This is unsurprising given that in contemporary society young people are increasingly required to be active managers of their lives and responsible for producing their own sense of identity (Giddens, 1991; Melucci, 1996; Furlong & Cartmel, 1997; Kelly, 2006).
As such, they commonly differentiate themselves from dependent drug users and resist any possibility that their AOD use is problematic (Muck, Zempolich, Titus, Fishman, Godley et al., 2001; Chassin, 2008). This has proven to be the case even when AOD use is closely connected with highly problematic life experiences (Rosenthal, Mallett, Milburn & Rotheram-Borus, 2008). This could go a long way to explaining why young people are generally far less likely than adults to access treatment services. As Room (2005) explains, this can be “…humiliating evidence of failure in self-management” (p151).
Duff (2003) recognises that contemporary youth culture in Western societies has produced the well- adjusted, responsible adolescent “…who uses drugs recreationally, very deliberately and very strategically” (p435). Such young people manage to stay integrated with a cultural mainstream (through education, employment, etc) and seldom come to the attention of AOD services.
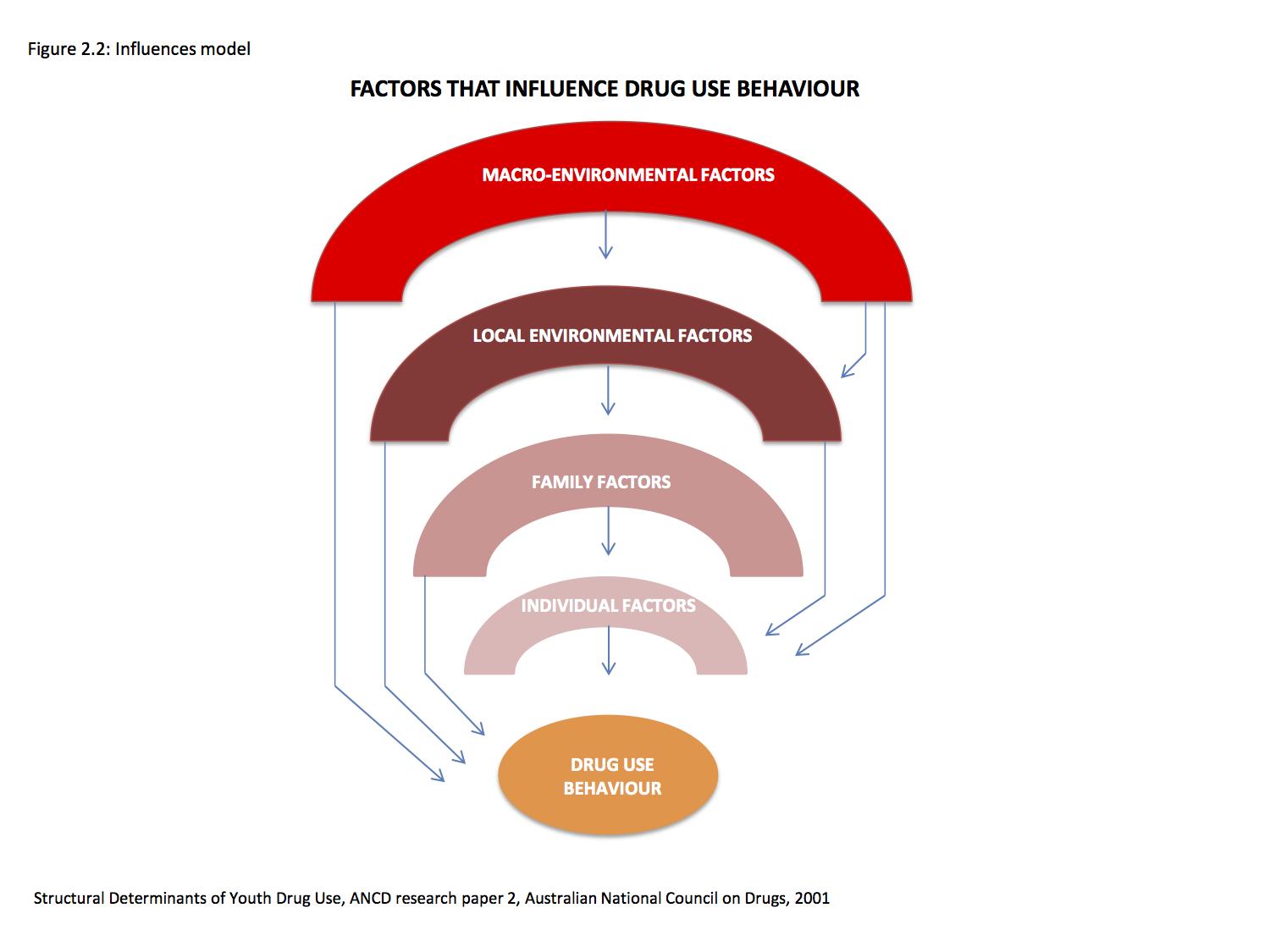
For other young people the demarcation between recreational and problematic use is less clear, being determined by a range of intrapersonal and socio- ecological factors that are often beyond their control (Measham & Shiner, 2009). The ‘influences model’ (Spooner et al., 2001) describes how such factors operate at multiple levels to shape the AOD-using behaviour of individuals (see Figure 2.2). Each level is associated with several factors.
- Macro-environmental factors include legislation, law enforcement, availability, and social ‘messages’ about use, e.g. via the media.
- Local environmental factors include traumatic experiences (e.g. child abuse, war, refugee camp), socio-economic status, support (e.g. peers, community), peer influences and labelling.
- Family factors include ineffective parental family management techniques, negative communication patterns, and poor family relationships and parental role-modelling.
- Individual factors include genetic predisposition, behaviour under control, personality (lack of social bonding, alienation, high tolerance of deviance, resistance to authority), knowledge about drugs, coping skills, commitment to education/academic problems, and early age of first use.